| About Fungitell The Fungitell kit is a highly sensitive, rapid diagnostic test that detects (1-3)-β-D-glucan in serum in as little as one hour. The Fungitell assay's ability to detect picogram levels of (1-3)-β-D-glucan in serum assists clinicians in identifying Invasive Fungal Disease (IFD) early in the disease process. Overview The Fungitell assay measures levels of (1-3)-β-D-glucan in serum. The detection reagent is a biological cascade based upon modified Limulus Amebocyte Lysate (LAL), an extract of the blood cells of the North American Horseshoe Crab. The assay is based upon a modification of the LAL pathway. The Fungitell reagent is modified to eliminate Factor C and, thus bypassing the activated factor B, to only react to (1-3)-β-D-glucan, through the Factor G-mediated side of the pathway. This renders the reagent highly specific for (1-3)-β-D-glucan and does not react to other polysaccharides, including beta-glucans with different glycosidic linkages. Enzyme Cascade 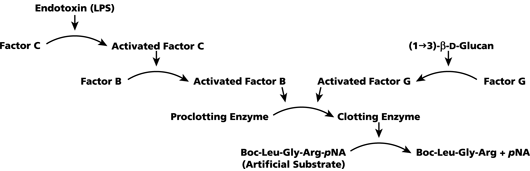 When (1-3)-β-D-glucan is present in a sample, it activates Factor G, a serine protease zymogen. The activated Factor G converts the inactive proclotting enzyme to the active clotting enzyme, which in turn cleaves pNA from the chromogenic peptide substrate, Boc-Leu-Gly-Arg-pNA, creating a chromophore that absorbs at 405 nm. The reagent is used in the Fungitell kinetic assay, to detect the rate of optical density increase in a sample. This rate is interpreted against a standard curve to produce estimates of (1-3)-β-D-D-glucan concentration in the sample. Similar to enzyme immunoassays, the Fungitell assay is performed in microplates and read in an incubating reader. Unlike standard enzyme immunoassays, however, the Fungitell assay does not require any washing steps. All reagents added remain in the well. It can be completed in approximately one hour. In May, 2004, the FDA cleared the Fungitell kit for sale, to assist in the diagnosis of fungal infections. The Fungitell assay was also CE marked for sale in Europe in March of 2008. Clinical Significance There is an increasing incidence of fungal infections by both primary and opportunistic pathogens, especially in immunocompromised patients. Invasive fungal diseases, as opportunistic infections, are common among hematological malignancy and AIDS patients and account for a growing number of nosocomial infections, particularly among organ transplant recipients and other patients receiving immunosuppressive treatments. Common primary human fungal pathogens are Candida spp. and Aspergillus spp., opportunistic fungal pathogens, including Fusarium spp., Trichosporon spp., Saccharomyces cerevisiae, Acremonium, Coccidioides immitis, Histoplasma capsulatum, Sporothrix schenckii and Pneumocystis carinii. The (1-3)-β-D-glucan produced by these organisms can be detected by the Fungitell assay. Normal human serum contains low levels of (1-3)-β-D-glucan, typically 10-40 pg/mL, presumably from commensal yeasts present in the alimentary canal and gastrointestinal tract. Most pathogenic fungi have (1-3)-β-D-glucan in their cell walls and minute quantities are sloughed into the circulation during the life cycle. Thus, (1-3)-β-D-glucan appears in the serum in cases of invasive fungal infection (IFI). Monitoring serum glucanemia for evidence of elevated and rising levels provides a convenient surrogate marker for IFI. Levels above 80 pg/mL, in at-risk patients, are considered positive. The Fungitell assay is indicated for presumptive diagnosis of fungal infection. It should be used in conjunction with other diagnostic procedures. The Fungitell assay does not detect certain fungal species such as the genus Cryptococcus, which produces very low levels of (1-3)-β-D-glucan. This assay also does not detect the Zygomycetes, such as Absidia, Mucor, and Rhizopus, which are not known to produce (1-3)-β-D-glucan. Patient Samples Serum samples should be collected in sterile vacuum tubes, allowed to clot, and then centrifuged to separate the clot from the serum, i.e., for approximately 1800 rpm for 10 minutes in a clinical centrifuge. Remove the serum sample under asceptic conditions and aliquot to storage vials. Each patient test requires .5 mL of serum. Serum is the only sample type that is currently approved for use with the Fungitell assay. Serum that is hemolyzed, lipemic, or visually icteric or turbid is not suitable for use with the Fungitell assay. Because a fungal infection is a dynamic process repeat testing, typically 2-3 times per week, improves sensitivity. Reference Values
| - | | <60 pg/ml | | ? | | 60-79 pg/ml | | + | | >/=80 pg/ml | The Fungitell assay is indicated for presumptive diagnosis of fungal infection. It should be used in conjunction with other diagnostic procedures. The Fungitell assay does not detect certain fungal species such as the genus Cryptococcus, which produces very low levels of (1-3)-β-D-glucan. This assay also does not detect the Zygomycetes, such as Absidia, Mucor, and Rhizopus, which are not known to produce (1-3)-β-D-glucan. Fungitell Kit
5,6 mL/vial, 2 vials/pack
|